 Hundreds of thousands of dogs have been treated by TPLO surgery for cranial cruciate rupture and a lesser number, but still well into the same order of magnitude by a decade younger TTA. Notwithstanding some recent, unfounded claims as to the more favorable outcomes of TPLO, both procedures, when executed properly, can compensate for the instability of the stifle with cruciate rupture. Not surprisingly, since the biomechanical basis is, in fact, the same – to modify the geometry of the joint so as to make the joint compressive force approximately perpendicular to the common tangent of the condyles in full extension where the risk for subluxation in the sagittal plane is the highest.
Hundreds of thousands of dogs have been treated by TPLO surgery for cranial cruciate rupture and a lesser number, but still well into the same order of magnitude by a decade younger TTA. Notwithstanding some recent, unfounded claims as to the more favorable outcomes of TPLO, both procedures, when executed properly, can compensate for the instability of the stifle with cruciate rupture. Not surprisingly, since the biomechanical basis is, in fact, the same – to modify the geometry of the joint so as to make the joint compressive force approximately perpendicular to the common tangent of the condyles in full extension where the risk for subluxation in the sagittal plane is the highest.
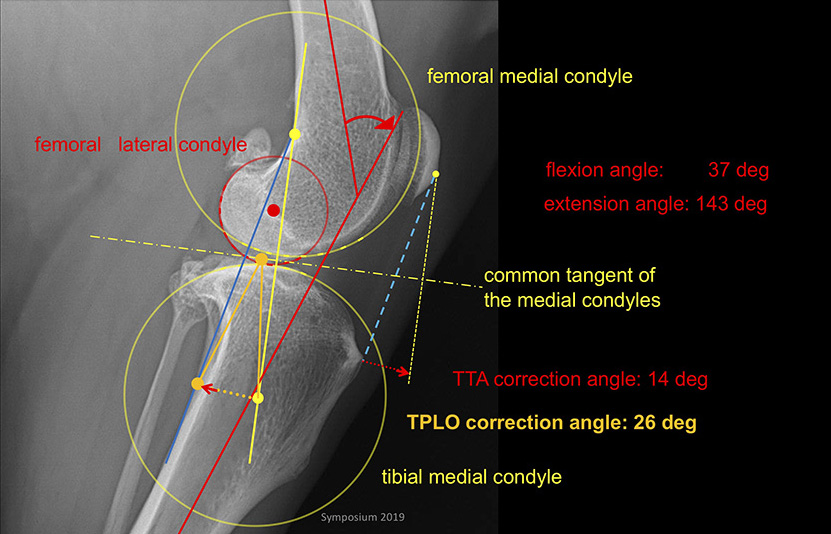
The intriguing question then is why TTA on average requires 12 degrees of rotation (achieved by rotation of the patellar tendon due to tuberosity advancement) compared to 20 degrees of rotation in TPLO (achieved by rotation of the tibia segment proximal to the osteotomy)?
This question has led us to examine the details of TPLO planning and premises involved in it. As it turned out, there are two major errors, which by coincidence approximately cancel each other, reducing the error to the level where crude measures of outcomes fail to detect the problem. One error is in the assumption that the joint force acts along the tibia long axis (simply impossible, in view of even a simple analysis by inspection of muscle forces involved); the other is in assuming that the tibia condyles are planar, whereas they are in fact convex with the radius of curvature about 50% larger than that of the femoral condyles. The good news, other than the luck of this error cancellation, is that planning for TPLO can be rationally based and thus – time will tell – possibly reduce the risks of problems in cases where statistics suggest they may come at the tails of distribution around the mean overcorrection of about 3 degrees but getting into two digits of over-corrections and somewhat less than that of under-corrections.
I have presented these arguments and the planning procedure on several occasions in the past two years and a manuscript has recently been submitted for publication. The video of my presentation at the Kyon 2019 symposium in Boston is embedded below. The Figure below suggests what we deem is an acceptable difficulty of rational TPLO planning provided that the lateral view of the stifle is taken in extension as required for TTA. With stifle flexed it is not possible to rationally plan for any procedure that involves shapes of two bones meeting at the stifle at risk of instability in extension and it certainly is not possible to base such a plan on one bone only. However, some luck and empirical surrogates have made both of these procedures the main drivers of growth and success of veterinary orthopedics in the last decades.